Frequently
Asked Questions
Table of Contents
![]() What is meningococcal disease?
What is meningococcal disease?
![]() What are the signs and symptoms?
What are the signs and symptoms?
What is
Meningococcal disease?
Meningococcal disease is a severe infection that
occurs when the meningococcal germ ‘invades’ the body from the throat or nose.
It does not occur in the people who carry the germ but rather occurs in people
who have very recently (within the previous 7 days) Acquired the germ from a
healthy ‘carrier’.
Meningococcal disease occurs in two main forms or it
can occur as a combination of these two forms. Meningococcal septicaemaia
occurs when the germ invades the bloodstream and causes blood poisoning.
Meningococcal meningitis occurs when the the germ infects the outer lining
around the brain and spinal cord.
What is the meningococcus?
The meningococcus is a bacterium that can be found at the back of the
throat or in the nose in about 10% of the community at any given time. Although
most people who ‘carry’ this germ in their throat or nose remain quite well,
they are able to spread it to others, a few of whom may subsequently become
very ill. It is spread in the fine droplets that are shed through coughing,
sneezing and spluttering
Back to
top
Who is at risk?
Anyone, anywhere can contract meningococcus, but those
most at risk are children under 5 years, teenagers and young adults, and older
people. Most cases are isolated and not
related to another case or an ‘outbreak’.
Back to
top
Background
Meningococcal
disease presents as meningitis, or rarely, as chronic meningococcemia or septic
arthritis. The disease is usually characterised by the appearance of a rash,
which progressively forms larger spots, which may merge into lesions. Petechial
rash in association with sudden onset of fever, headaches and stiff neck,
vomiting and drowsiness is highly suggestive of meningococcal meningitis. The
causative agent is a gram-negative diplococcus, Neisseria meningitidis,
of which there are 13 known serogroups, each having a different capsular
polysaccharide. Over 90 per cent of meningococcal disease is caused by
serogroups A, B or C.
Spread of infection
Transmission of Neisseria meningitidis is primarily via respiratory droplets from the nose and throat of an infected person. The organism may be asymptomatically carried by up to 25 per cent of the community, and only a few of these will develop invasive disease. It may cause sudden serious illness and death in a previously healthy person, and as a result can cause considerable anxiety and panic in a community.
Close contact with a person who has meningococcal disease poses an increased risk of infection; the relative risk compared to the general population can be greater than 1000. The risk of infection from a case to contacts may persist for many months, but the greatest risk is during the first five weeks following the onset of disease in the index case (original case).
Meningococcal disease is most frequently seen in winter and early spring.
Upper respiratory tract infections particularly those caused by influenza A may
increase the risk of invasive meningococcal disease.
Vaccines
A vaccine against meningococcal groups A, C, W135 and
Y can be given to people traveling to areas of the world where these strains
occur, has been available to some years.
I t is effective in about 80% of those who receive it, but it is not
effective in children under the age of 18 months and only offers protection for
about 3 years.
A new, more effective conjugated vaccine for the
meningococcal C strain is available in Australia. This vaccine can potentially protect infants and children, as
well as adults, and offers immunized individuals longer-term protection against
meningococcal C disease. Clinical
experience in the UK has confirmed the value of this vaccine in reducing
outbreaks of this disease among paediatric populations.
There is no vaccine against meningococcal group B,
which is still the most common group causing meningitis and meningococcal
septicaemia.
Awareness of the signs and symptoms of meningitis and
septicaemia, and being prepared to take action swiftly is very important.
What
are the signs and symptoms?
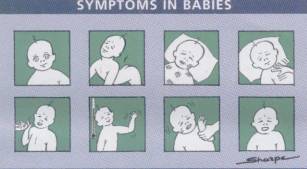
Symptoms in babies:
Ø
High
temperature, fever and possibly hands and feet cold.
Ø
Refusing
feeds and/or vomiting.
Ø
Crying,
high pitched moaning and fretting.
Ø
Aversion
to being handled.
Ø
Arching
of the back and neck arched.
Ø
The
fontanelle can be bulging or firm. A blank, staring expression.
Ø
Difficult
to wake.
Ø
Blotchy
and pale complexion.
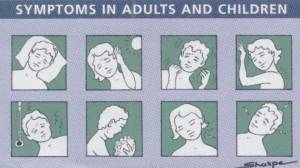
Symptoms in children and adults:
Ø
Vomiting.
Ø
High
temperatures, fever possible with cold hands and feet.
Ø
Extreme
headache.
Ø
A
severely stiff neck.
Ø
An
aversion to light and lighting.
Ø
Being
drowsy.
Ø
Joints
and muscles aching.
Ø
Fitting.
Prompt diagnosis of meningococcal
septicaemia and meningitis and preadmission treatment of
presumptive cases can be life saving.
Treatment & prevention
Bacterial
meningitis and meningococcal septicaemia demand immediate treatment with
antibiotics.
Only people who
have come into close contact with patients suffering from bacterial meningitis
and meningococcal septicaemia require antibiotics. (Close contacts are people
living or sleeping in the same household or who have intimately kissed the
patient.) School friends and work mates
of the patient with meningococcal disease are rarely at higher risk unless
several cases occur together.
Antibiotics are
given to kill off any meningococcal bacteria, which may be carried in the back
of the nose and throat. This reduces
the risk of passing the bacteria on to others.
Research suggests that smoking in the household setting may increase the
risk of a child contracting bacterial meningitis.
Apart from
vaccines, there is no known way to protect against meningitis and meningococcal
septicaemia.
Viral meningitis
does not respond to antibiotics; treatment is based on rest and good nursing
care.
Where to get help
- Your doctor
- Emergency department of your local
hospital
- Disease Control Section, Public
Health and Development Division, Department of Human Services Tel. (03)
9637 4126
After
you have seen a doctor, if your child or friend becomes more unwell or you
continue to be worried, seek further help.
Last revised: Date